

The best way to look inside your uterus is by having a hysteroscopy. This examination of the uterine cavity allows your specialist to visualise the lining and cavity in real time rather than relying on scans that look at the womb from the outside.
You get a straight answer as to whether to explore irregular bleeding as part of a fertility evaluation before IVF. The operation is straightforward: A small, lighted hysteroscope is softly inserted through the cervix, allowing a detailed view of the womb, without a single cut in the abdomen.
On this page, you will find what can be seen during a hysteroscopy, your options for anaesthesia, and what your day-care recovery includes at Zivah. Here's what a camera inside the uterus reveals that external scans routinely miss.
What Is a Hysteroscopy? (Hysteroscope Definition & How It Works)
A hysteroscopy, sometimes shortened to HSC in clinical notes, is a direct look into your uterus. It uses a hysteroscope, a thin, lighted tube with a tiny camera at the tip. The plain meaning of hysteroscope is simple: it’s a thin telescope or camera for the womb. This uterine scope is carefully inserted via the cervix and transmits a live image to a screen so your doctor can view the cavity in real time.
This is the basic difference from a scan. An ultrasound or X-ray only shows the womb from the outside; a hysteroscopy shows it from the inside. This is how inserting a camera into the uterus is seen as minimally invasive gynaecology, or gynaecological endoscopy, because nothing larger than the scope goes into the body.
Hysteroscopic View: What the Camera Sees Inside the Uterus

But what does the hysteroscopic view really show? Once entered, the camera visualises the whole uterine cavity. Your specialist looks at three key things:
- The endometrial lining - the layer where an embryo will implant
- The cavity contour - its overall size and shape
- The tubal ostia – tiny holes where the fallopian tubes connect to the uterus
During hysteroscopy, a normal uterus will have a smooth uniform lining, a clear triangular cavity and both ostia visible. In contrast, hysteroscopy findings that get flagged may include a thicker lining, a polyp or fibroid, scar tissue, or an unusual shape, which are the signals that commonly explain abnormal bleeding or fertility issues.
Diagnostic vs Operative Hysteroscopy
This creates an important distinction. Diagnostic hysteroscopy is just for looking; the diagnostic hysteroscope is used to examine, identify the cause, and plan the next step.
An operational hysteroscopy is more advanced. If any problem is found, such as a polyp or fibroid, fine instruments are passed via the same scope and the problem is treated there and then.
| Feature |
Diagnostic Hysteroscopy |
Operative Hysteroscopy |
|---|---|---|
| Purpose |
Inspect the cavity to find a cause |
Inspect and treat in the same session |
| Common use case |
Abnormal bleeding, fertility workup, unclear scan result |
Removing polyps, fibroids, adhesions, or a retained IUD |
| Typical duration |
About 5–15 minutes |
About 15–60 minutes or more |
This is known to clinicians as the ‘see-and-treat’ strategy, which typically means a separate hysteroscopy operation on another day isn’t needed.
Why Hysteroscopy Is Recommended: What a Hysteroscopy Can Detect
Why would your specialist suggest a hysteroscopy? It shows things other tests don’t. When symptoms or scans don’t match up, a hysteroscopy looks right inside to get a clear picture of the uterine cavity. What does a hysteroscopy show? It is most typically used for:
- Evaluation of abnormal uterine bleeding - heavy periods, spotting, or bleeding after menopause
- Suspected intracavitary lesions - growths within the cavity (e.g. polyps, fibroids)
- Infertility workup - How to assess the health of the womb when conception is difficult
In short, it is the most direct way to confidently diagnose abnormalities in the uterus and to identify intrauterine pathology that imaging may merely suggest.
Hysteroscopy for Fertility, Pre-IVF & Recurrent Loss
This is where hysteroscopy comes into play, especially for those considering pregnancy. This is why a uterine examination before IVF counts; a healthy cavity is the basis for a successful embryo transfer. At Zivah, it’s a specialised test for fertility to examine the health of the womb before treatment. Your specialist will check your endometrium before embryo transfer by:
- Endometrial assessment (the lining for implantation)
- Both fallopian tubes are patent and open
- Screening of chronic endometritis, a low-grade inflammation of the lining
- Diagnoses and treats Asherman’s Syndrome (intrauterine adhesions)
This uterine health screening for pregnancy planning is used to evaluate Repeated Implantation Failure (RIF) and Recurrent Pregnancy Loss (RPL). It is an important part of any implantation failure or recurrent miscarriage workup.
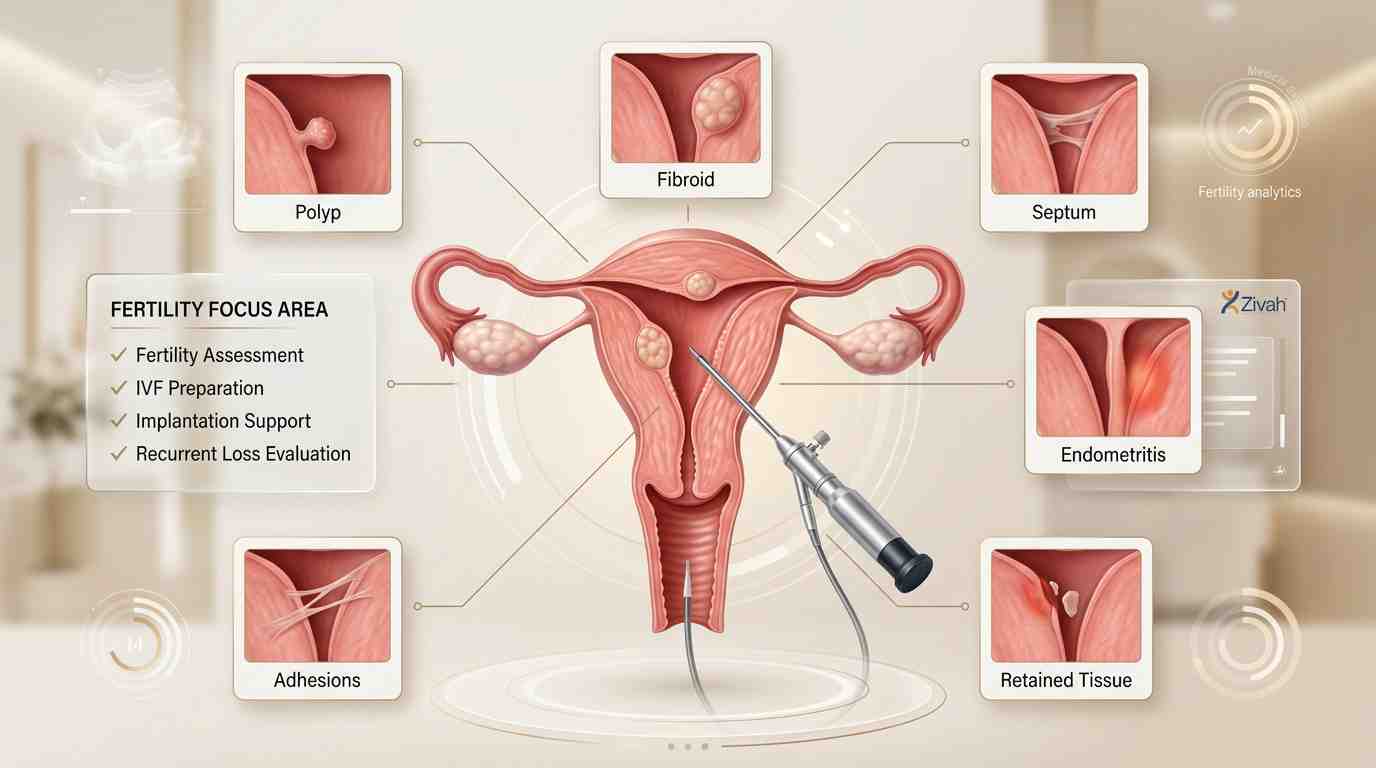
Uterine Findings That Affect Fertility & Their Hysteroscopic Management
| Finding |
Impact on Implantation / Fertility |
Hysteroscopic Action |
|---|---|---|
| Endometrial polyp |
Can block implantation or cause bleeding |
Polypectomy (removal) |
| Submucosal fibroid |
Distorts the cavity and lowers implantation |
Hysteroscopic myomectomy |
| Intrauterine adhesions (Asherman's) |
Scar tissue thins the lining and can cause loss |
Adhesiolysis (scar release) |
| Uterine septum |
Linked to miscarriage and recurrent loss |
Septoplasty (septum resection) |
| Chronic endometritis |
Inflamed lining lowers receptivity |
Diagnosis + guides antibiotic treatment |
| Retained tissue / displaced IUD |
Causes bleeding and blocks conception |
Targeted removal |
Uterine Conditions Diagnosed and Treated
Hysteroscopy is also used to diagnose and treat a variety of uterine disorders, all in one visit, beyond fertility. It is used for diagnosing womb polyps (soft growths on the lining) and submucosal fibroids (muscular growths that push into the cavity).
It also recognises intrauterine adhesions, the scar tissue of Asherman's Syndrome, and a uterine septum, a wall of tissue present from birth that separates the cavity. The same technique can be used for the removal of retained pregnancy tissue and displaced IUDs.
Who Should Not Have a Hysteroscopy
Is hysteroscopy right for everyone? Not exactly. To minimise the risks of hysteroscopy, it is not conducted if you are pregnant or might be pregnant, if you have a current pelvic infection, or if you have confirmed cervical or endometrial cancer. Heavy bleeding can also obscure vision; therefore, the timing may have to be altered. First, your specialist will check that you're a good candidate.
Preparation for Hysteroscopy and Procedure Timing
It’s easy to get ready for a hysteroscopy. Preparing for hysteroscopy starts with your medicines; tell your expert all the things you take, including vitamins and supplements. A few days prior, you may need to stop your blood thinners or aspirin (anticoagulants).
A pregnancy test is routine, as the procedure is not done during pregnancy. If you get general anaesthesia, you will be asked to fast for many hours beforehand; if you are sedated, arrange a ride home.
Best Time in the Cycle for Hysteroscopy
When is the best time for hysteroscopy? The best time for a hysteroscopy during routine cycles is the first week after your period has finished. The lining is thin at this time, offering the best view of the cavity, and there is no risk of an early pregnancy.
Your hysteroscopy will not be performed during your period (menstruation) as the blood may block the view of the camera. It can be done any time after menopause, and the timing is variable.
Consolidated Hysteroscopy Prep & Timing Checklist
| Before the Procedure |
On the Day |
What to Avoid |
|---|---|---|
| Share all medicines & supplements |
Empty your bladder before you start |
Sex, tampons, or douching 24 hrs before |
| Pause blood thinners/aspirin if advised |
Wear loose, easily removed clothing |
Eating or drinking if under general anaesthesia |
| Schedule after your period, before ovulation |
Arrange a ride home if sedated |
sedatedBooking during active menstruation |
Hysteroscopy Anaesthesia and What Happens During the Procedure

Are you going to be put to sleep for a hysteroscopy? Not always. The type of hysteroscopy anaesthesia will depend on the situation. A basic diagnostic scope done in the office often requires only local anaesthetic, or even hysteroscopy using the mild "no-touch" approach without anaesthesia at all.
If you need an operation, you can have a hysteroscopy while being unconscious or under general anaesthetic, so at Zivah, you will always be kept completely comfortable and sleeping if required. Here's what occurs, in order:
- You lie on your back with your feet on supports, and the area is gently cleaned.
- A hysteroscope or thin lighted hysteroscopy scope is introduced through the cervix into the uterus.
- They push warm saline into the cavity to open it and clear the view.
- Your specialist examines the lining, cavity and tubal apertures on a screen.
- Fine hysteroscopy instruments are used in the same scope if therapy is required.
The scope is then out, and most diagnostic visits take only minutes.
Hysteroscopy Recovery: Recovery Time and Aftercare
Most people are surprised by how quick hysteroscopy recovery is.A diagnostic hysteroscopy is an outpatient procedure, so you will go home the same day. There may be some light spotting and mild cramps for a few days. Recovery time for hysteroscopy is quick, and many women feel back to themselves within 24 hours.
Simple hysteroscopy aftercare includes wearing pads, not tampons as you spot, and avoiding baths, swimming and hot tubs for a little while. Hysteroscopy D&C recovery is comparable to hysteroscopy and D&C or resection recovery, with a slightly longer pelvic-rest period. Recovery following a purely diagnostic hysteroscopy is quicker.
And intercourse? Sex after a hysteroscopy is usually put on hold until the bleeding stops, which is usually approximately two weeks or as recommended by your expert.
Hysteroscopy Recovery Timeline: What's Normal & When to Contact Zivah
| Timeframe |
What's Normal |
When to Contact Zivah |
|---|---|---|
| Same day |
Mild cramps, drowsiness if sedated |
Heavy bleeding or feeling very unwell |
| First few days |
Light spotting, period-like cramps |
Severe abdominal pain |
| 1–2 weeks |
Spotting eases, normal activity resumes |
Fever or chills |
| First cycle |
Period returns, may feel slightly off |
Foul-smelling discharge |
But generally, your period following hysteroscopy is on time. The first cycle may feel a little odd. And can you get pregnant after hysteroscopy? Yes, the treatment can really boost your chances by cleaning the cavity. Your team will let you know when it's safe to start trying.
Risks and Side Effects of Hysteroscopy

How safe is hysteroscopy? Very much so. The procedure is generally thought to be safe, and major problems that can happen during hysteroscopy are very uncommon (less than 1 in 100 cases).
For most patients, the side effects of hysteroscopy are modest and short-lived. You may experience some mild spotting or bleeding for a few days, some period-type cramping, or feel a little sick or queasy immediately after.
These side effects normally go away on their own in a day or two. As with other procedures, there are rare risks with hysteroscopy. Some of these are:
- An infection that is cured by antibiotics
- Uterine perforation: A tiny tear in the wall of the uterus
- Heavier bleeding than expected
- Reaction to the fluid used to open the cavity, or anaesthesia
The most prevalent, though still rare, is uterine perforation, which normally heals on its own. Your specialist will assess your health beforehand and monitor you during your hysteroscopy to make sure it is safe. If you see a fever or a lot of pain or a lot of blood afterwards, call your team.
Hysteroscopy Report Terminology Decoder
Your hysteroscopy report should not be a foreign language to you.You will be given a brief overview of what was found during your hysteroscopy after your procedure. Normal hysteroscopy means the inside of your uterus looks normal. Below are the terms that describe each phrase in plain English, so you can see what your results mean at a glance.
Hysteroscopy Report Terms Explained
| Report Term |
What It Means in Plain Language |
|---|---|
| Normal cavity |
A healthy uterus shape with a smooth lining, a normal uterus on hysteroscopy |
| Endometrial thickening |
The lining is thicker than expected and may need a closer look |
| Polyp |
A small, soft growth on the lining |
| Submucosal fibroid |
A muscle growth pushing into the cavity |
| Synechiae / adhesions |
Bands of scar tissue inside the uterus (Asherman's Syndrome) |
| Septate uterus |
A wall of tissue dividing the cavity, present from birth |
| Patent ostia |
The fallopian tube openings are clear and open |
If the hysteroscopy shows a normal uterus in your report, then usually no additional treatment is required. If something is flagged, your professional will guide you through the next step.
Hysteroscopy at Zivah: Brand Strengths & Next Steps
Hysteroscopy is when your physician can see as clearly as possible inside the uterus to diagnose, confirm a healthy cavity, or treat a problem in one go. That is the kind of care Zivah is built for. The technique is minimally invasive, and recovery is rapid and comfortable.
Because of its see-and-treat strategy, diagnosis and treatment are typically combined, saving you a return visit. And for those considering pregnancy, it plays a direct role in improving endometrial receptivity, preparing the womb for the best chance of implantation.
If you've been referred for a hysteroscopy, the next step is easy: reach out to the Zivah team to discuss your options and schedule a consultation that works for you.
Cost of Hysteroscopy at Zivah
Curious about how much a hysteroscopy may cost? Depends on a few variables. The final fee varies by type of operation; a rapid diagnostic hysteroscopy costs less than an operative procedure to address a polyp or fibroid in the same visit.
Your anaesthetic can also make a difference, as local or no anaesthesia is very different from a general anaesthetic. Any additional steps, such as biopsy or resection, may affect the total. To get a clear personalised quotation, just contact Zivah's billing desk.